To repair or not to repair hernia?
To Your Good Health
DEAR DR. ROACH: For many years, I have had a visible abdominal hernia that is above and to the right of my belly button.
My primary doctor declared it an “incisional hernia,” probably due to gallbladder surgery from many years ago. He declared that surgical repair was entirely optional. Annual examinations did not change his diagnosis.
I’ve never had pain or discomfort from it, and I have no problem eliminating it. Notably, I can maneuver 50-pound luggage in and out of our SUV (not easily but without pain). I was due for my final colonoscopy (I’m 76), and when my gastroenterologist saw it, he indicated — fairly stridently — that it must be repaired.
I went for a scan with contrast, and he stated that the result supported his determination. He had to end the colonoscopy early due to his inability to get the scope past the hernia. All previous colonoscopies had been completed normally.
So, I went to the recommended surgeon in the medical group. He examined me, and the scan determined that no repair was necessary. I was thrilled since the required “mesh” repair scares me.
— G.L.
ANSWER: A hernia is a defect in the abdominal wall. If a defect is large enough, abdominal contents, including the small and large bowel, can come through this defect.
If they get trapped (“incarcerated”), then this is considered a surgical emergency as they can get swollen and stuck, then lose blood, leading to profound cell death and requiring lifesaving surgery. Preventing incarceration and relieving symptoms are the main reasons to perform a surgery.
In my mind, the surgeon is the definitive expert on determining the need for surgery, and this is especially true for hernia surgery.
In general, asymptomatic abdominal wall hernias do not need to be repaired. These include umbilical hernias (which are related to an embryological space that has stretched during a lifetime) and incisional hernias (where the abdominal wall reopens after surgical closure).
A CT scan can confirm that there is a hernia, and I have no doubt that the abdominal contents had moved through the hernia at the time of the scan. This was probably the case during the colonoscopy as well, which made it impossible to do the procedure.
However, the fact that the hernia has been asymptomatic for many years is reassuring; the likelihood of an emergency due to your hernia is very small.
Dr. Roach regrets that he is unable to answer individual letters, but will incorporate them in the column whenever possible. Readers may email questions to ToYourGoodHealth@med.cornell.edu.
Lifestyles

Organ donation after heart stops gains popularity in US
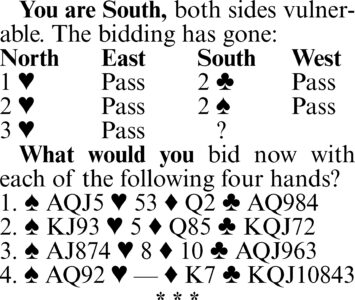
Bridge by Steve Becker
Mind Challenge trivia unfolds at senior centers
When was the first speeding ticket issued? This stumper prompted debate and some research from trivia teams ...
Hints from Heloise: Opening fruit cups without the mess
DEAR HELOISE: In response to the question about how to open fruit cups without spilling: Before opening it, tilt ...
Dear Annie: From retired accountant to uninvited inspector
DEAR ANNIE: My 72-year-old father retired from his accounting job two years ago and appointed himself “Director ...
